Psychiatry is a framework that assumes that human suffering can be categorized and treated as medical diseases and disorders. In Western countries, this is often the prevailing framework for dealing with suffering, and it may be treated as absolute truth.
You’re not just sad: you have depression, which means you need to take this medication and go to this therapy. You see things because you have schizophrenia, so you need to take this medication for the rest of your life to stop seeing things. Your pain has nothing to do with the trauma inflicted on you throughout your life. It’s a brain disease- unless, of course, it is the trauma. Then it’s post-traumatic stress disorder, but only if you struggle with it in a specific way. And even then, there’s a track to get on, a set idea of what Recovery is Not Absolute is supposed to look like.
There’s a solution for every problem… unless, of course, that problem isn’t well-studied or doesn’t fit into one of the many diagnostic categories. Then, you’re on your own. Good luck. We can’t help you.
For some people, psychiatry works. Medications and therapy can and do help make life easier to cope with, help dull oversensitivities and lift mood. They can stabilize someone swinging wildly out of whack.
The trouble is that psychiatry is just another framework, and it may or may not have objective truth to it. It’s a lens to view pain through, but the categories we place that pain into were defined by human beings just like anything else. We treat it as something that works for everyone when the reality is that it doesn’t always do the job. Still, we cling to the notion that it will save us all if we try a little harder to make it work.
If diagnostic categories were objective and absolute, if every condition had a clear-cut cause and diagnosis and treatment, if that system always worked like we think it works- if that were the case, then folks interacting with the psychiatric system wouldn’t be suffering. It would be effortless to fix that pain. Take these meds. Follow this track. And yet there are a good number of people having to find their own way despite having plenty of encounters with the psychiatric system. The system didn’t work for them.
The framework works for some people (good for them!), but the fact that it hurts or has no effect on others says something about its nature. Psychiatry is not a perfect system. If it works for you, great! Keep using it. The framework does exist for a reason. Just as importantly, if it isn’t working, discard it and try something else.
Context: Emil Kraepelin is credited as being one of the first people to establish assumptions underlying psychiatry.
Through Kraepelin’s life and afterwards, the field of psychiatry continued to gain political power, and for many years now, it has been generally considered to be the highest authority in the field of mental health in the West, especially regarding the psychotic disorders such as schizophrenia.
(Raised the question: does it have to be the highest authority? What was there before psychiatry?)
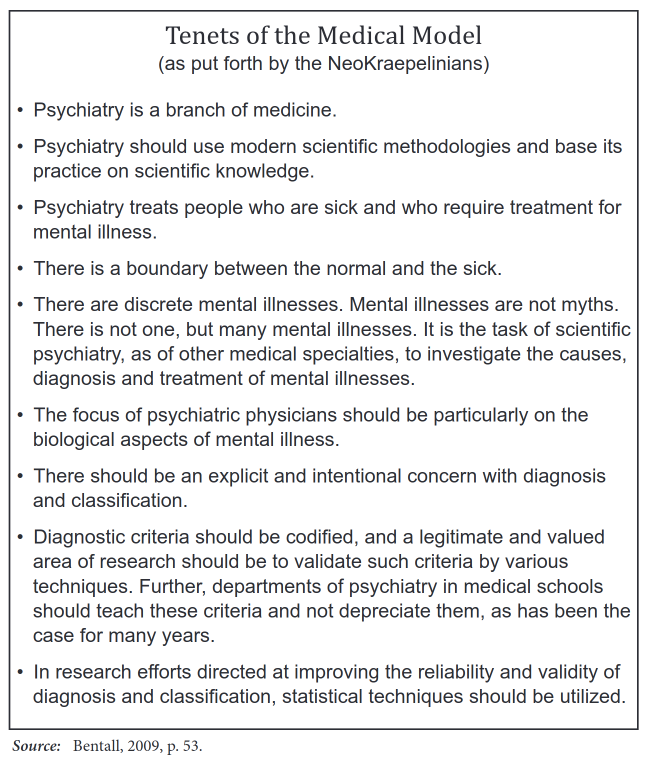
Although these principles are rarely articulated as clearly as they are here, it is evident that they continue to lie at the foundation of the dominant paradigm in the mental health field today, a paradigm that is often referred to simply as the medical model. When researching long-term psychotic disorders, it’s important to acknowledge that most of the assumptions we have in the West regarding the extreme states of consciousness to which we have given labels such as Psychosis, schizophrenia, schizoaffective disorder, bipolar disorder, etc., come directly from this model.
Dr. Paris Williams, Rethinking Madness: Toward a Paradigm Shift in Our Understanding and Treatment of Psychosis, 2012
How much of what we put down to the ‘mental illness’ is the stress of this way of living? The loneliness of it, the chronic, grinding fear?
Sarah K Reece, Happiness, 2014
During the ’70s and ’80s, trauma and child sexual abuse were assiduously ignored by most professional therapy schools and the big academics. They pretended it didn’t exist. It was actually an activist grassroots movement that forced the schools to recognize how crucial trauma and specifically childhood sexual abuse is in the psychological development of many.
The evolution of our understanding of PTSD is very similar. The major academic institutions denied that it existed for a long time. It was the Vietnam veterans’ rap groups who knew this stuff happened. They got together and, with the help of psychiatrist Robert Jay Lifton, organized a movement and put political pressure on the government. It was this pressure that forced the academics to accept PTSD as something real and forced them to include the diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, which is the bible of psychopathology in academic America.
So, these big changes have occurred within my lifetime. Having watched this process with child sexual abuse and PTSD has given me a healthy skepticism about the academic authorities on psychological healing. Despite all the degrees, high academic honors, and position, they have been fundamentally and disastrously wrong about the basics of psychological healing.
Falconer, The Others Within Us